A fragrance free bug spray
Finding a fragrance free bug spray can be quite a challenge… this is one that is designated by the manufacturer as “no fragrance”
Finding a fragrance free bug spray can be quite a challenge… this is one that is designated by the manufacturer as “no fragrance”

On June 23, 2016, a historic event occurred – the first US Nickel Workshop. Thought leaders from medicine, industry and regulation came together to discuss the issue of nickel dermatitis, appropriate uses of nickel, and the integral role of nickel in society at the first North American Workshop on Nickel Dermatitis. This workshop was sponsored and coordinated by the Nickel Institute, who brought toxicologists and dermatologists together with conscientious companies representing various consumer product sectors. The group stressed the importance of nickel release, not nickel content in determining risk of becoming allergic to nickel and having a nickel dermatitis reaction if you are already allergic to nickel.
Removing nickel from our environment is not possible, because it is one of the most abundant metals on our planet and it has many beneficial uses where it cannot be reasonably substituted (e.g. stainless steel) . What is possible, though, is to use it in the safest ways possible. For example, nickel is safely used in several types of stainless steels. Nickel is also used as nickel-plated carbon fibers in the composite case of personal cell phones to keep our brains safe from the electromagnetic energy generated from by cell phone use. A top priority was discussed at the nickel workshop of removing high nickel-release materials from use in piercing posts (used in jewelry) by using appropriate low nickel-releasing materials (e.g. surgical stainless steel, high quality gold, etc.) since piercing directly introduces releasednickel to an open wound. This is especially important for children who, if sensitized, have a lifetime to deal with the consequences.
The Nickel Institute will be putting together a full report from the Nickel Workshop, which will be made available online on the Nickel Institute website at https://www.nickelinstitute.org Dr. Jennifer Chen, MD, a dermatologist from Stanford University, presented the background of nickel allergy in the US at the Nickel Workshop in addition to developing an outreach education webinar on this topic available to the public https://www.dermatitisacademy.com/webinars/ The webinar discusses that EU regulations have decreased nickel allergy in ear pierced young women from 16.6% down to 6.9%. The estimated savings of $2 billion over the last 20 years is massive and that could translate into an even bigger savings with the US population.
At the Nickel Workshop, Dr. Sharon Jacob, MD, a dermatologist from Loma Linda presented the situation of nickel dermatitis in children in North America, noting that nickel allergy is found at an early age and is thought to be largely due to ear piercing in young girls. She reported that an estimated 11% of the US general population is currently sensitized to nickel, which includes an estimated 8,133,603 children! She also stated that a significant proportion of these could be prevented by utilizing safer metals in piercing. Dr. Jacob ended her presentation at the Nickel Workshop with a slide that said:
‘You can’t tell an adult they can’t pierce and smoke… but you can protect a child.’
To learn more about nickel allergy and sensitization, please visit the Dermatitis Academy page dedicated to nickel https://www.dermatitisacademy.com/nickel-page/ which includes information on the low nickel diet, how to DMG test metal objects to screen for nickel release, a quiz on sources of nickel and a general population questionnaire on nickel sensitization. https://emg.wufoo.com/forms/nickel-allergic-contact-dermatitis-survey/

The DMG has modest sensitivity:
“The sensitivity of the DMG test was 59.3% and the specificity was 97.5% based on DMG-test results and nickel release concentrations determined by the EN 1811 reference method. … The EN 1811, a European standard reference method developed by the European Committee for Standardization (CEN), is fine-tuned to estimate nickel release around the limit value of the EU Nickel Directive from products intended to come into direct and prolonged skin contact.”
Direct and prolonged contact with FREE RELEASED nickel is what leads to sensitization and skin rashes (allergic contact dermatitis). Because of the DMG sensitivity issue (not always detecting) – consumers should not rely on this 100% but rather use if for screening.
Past exposure studies may have underestimated nickel release from consumer items.”
Read more here:
http://www.ncbi.nlm.nih.gov/pubmed/20536475
From a clinical impact standpoint, if the object turns pink with the DMG test – best to avoid it – but be aware that it is not 100%… DMG sensitivity is only 59.3%
learn about DMG testing here:
https://www.dermatitisacademy.com/nickel-sources/
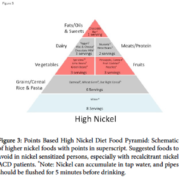
‘ A meta review by Jensen specifically assessed elicitation of SCD due to nickel ingestion, and found that 1% of those sensitized to nickel react to the nickel content of a “normal” diet, defined as 0.22 mg, 0.35 mg, or 0.53 mg [12]. Furthermore, a dose-response relationship was revealed showing 10% of nickel sensitized patients responding to exposures between 0.55 mg and 0.89 mg. Such low exposures can be easily attained by consuming foods high in nickel content. …many patients sensitized to nickel are unaware that dietary exposure may play a role in their morbidity.’ A low nickel diet may help them get their rashes better.
To read more about the Low Nickel Diet: A Patient-Centered Review click here:

Steroid allergy: I saw a patient with ‘recalcitrant eczema’ that was doing fairly well, flares here and there. Being told there’s nothing on my back – should mean exactly that – but when I checked – there was a 2+ positive reaction.
I can not stress enough how nice it is to have either a photo or a map of patch placement to be able to go back and figure out what chemical is causing that reaction…
So we aligned a ‘decoder’ grid – and lo and behold were able to identify the placement of budesonide, a class B steroid (steroid allergy). Asked about the current treatment regimen and low and behold the patient is using a class B steroid daily – well, we won’t be doing that anymore…
There are three corticosteroids on the Food and Drug Administration approved (for adults) patch test – they are a recognized allergens…https://www.dermatitisacademy.com/corticosteroids/
So, what is the surprise in this?
Well, the patient was patch tested by another provider 82 days earlier – the steroid had not shown up as a positive during the patch procedure week.
Is this commonly reported? No. could it have been potentially missed? Yes.
Conclusion – always watch for late delayed reactions and “flare up” responses… especially in steroid allergy, as steroids have anti-inflammatory properties.
Learn about one of the most important environmental campaigns in history…. the environmental working group studied cord blood samples and provide evidence that we are in the midst of a silent pandemic.
“Aught to do all we can to minimize exposures”… “industrial pollution begins in the womb”…”women use an average of about 12 personal care products a day and that exposes them to more than 160 chemical ingredients, some of them rather toxic, day after day after day”.
“62,000 chemical were ‘grandfathered in'”
“…found 287 chemicals in just those 10 Americans — 28 different waste byproducts — 47 different consumer product ingredients — most disturbing of all – 212 industrial chemicals and pesticide break down products that had been banned 30 years before… ” in UMBILICAL CHORD BLOOD! Speaking to the silent pandemic.
“babies are born pre-polluted with as many as 300 industrial chemicals in their bodies.” The math shows … “We have more health effects than we have chemicals, why is that? … many of these chemicals have multiple toxic effects.” And, “Only 5 chemicals have been banned or restricted by EPA under the law“! Moreover, “80% of all new chemicals approved within 3 weeks”
There is an “84% increase in acute lymphocytic leukemia“…
The Kid-Safe Chemicals Act (KSCA) of 2008 – “Requires that chemical be safe for CHILDREN and others who are sensitive”. “Assumes chemicals are harming people until PROVEN OTHERWISE“. “Prioritizes SAFETY REVIEWS, BANS, and PHASE-OUTS based on what’s in people and hazardous”. Addressing the silent pandemic.
…historic moment … AN UNPRECEDENTED COALITION!!!
Learn more:

Methylisothiazolinone scrutiny is very much needed. This preservative is sensitizing a significant number of adults and children worldwide. It is found in personal products, household cleaners, household paint, and air fresheners. Reactions to it may look like atopic dermatitis!
“Recalcitrant dermatitis, such as that of the hands, face, or genitals, may be due to allergic contact dermatitis (ACD) from ingredients in seemingly innocuous personal care products. Rising rates of allergy have been noted due to the preservative methylisothiazolinone (MI). This preservative is commonly found in skin and hair care products, especially wipes. This study evaluated the use of MI in products specifically marketed for babies and children and examined the associated marketing terms of such products. Ingredients of skin care products specifically marketed for babies and children were surveyed at two major retailers. Of 152 products surveyed, 30 products contained MI. Categories of products surveyed included facial or body wipes, antibacterial hand wipes, hair products, soaps, bubble baths, moisturizers, and sunscreens. Facial or body wipes and hair products were the categories with the greatest number of MI-containing products. MI-containing products were manufactured by a number of popular brands. Of note, products marketed as “gentle,” “sensitive,” “organic,” or “hypoallergenic” often contained MI, thus emphasizing the importance of consumer scrutiny of product choices. These findings reinforce the importance of educating parents and providing consumer decision-making advice regarding common skin care products, in order to help prevent ACD in children.” Learn more by clicking here: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4197884/.
It is time for methylisothiazolinone scrutiny – there is an epidemic! The Dermatitis Academy [www.dermatitisacademy.com] is tracking this epidemic and reporting new cases of methylisothiazolinone and new sources!!! It is important that consumers continue to let the Food and Drug Administration [FDA] know that they are known to be allergic to methylisothiazolinone and which product they have reacted to. Click here for information on FDA reporting: https://www.dermatitisacademy.com/methylisothiazolinone-page/
This is a duplicate posting with a different featured image.

By Hannah Hill, MD and Sharon E. Jacob, MD
It is time to be Simple & Free! Pediatric allergic contact dermatitis (ACD) has been increasingly recognized in the United States over the last decade. Reported rates of positive patch tests in children referred for suspected ACD range between 27% and 95.6%. Many young children are becoming sensitized to contact allergens found in personal hygiene products such as cleansers, moisturizers, sunscreens and topical medications like steroids and antibiotic ointments. Dr. Jacob and her team have been promoting pre-emptive avoidance strategy (P.E.A.S.) since 2005, especially in patients with widespread dermatitis, and seeing a remarkable impact. This led to the team developing the Simple & Free guideline, making P.E.A.S publicly available, with the goal of reducing skin rashes (dermatitis) associated with the top sensitizing allergens and potentially a decrease in sensitization.
With the goal of identifying the top allergens responsible for a significant portion of pediatric ACD caused by personal hygiene products, Hill et al. reviewed five recent pediatric patch test studies. The top ten allergens identified by this meta-analysis of the US pediatric patch test were neomycin, balsam of Peru (a screening substance for fragrance allergy), fragrance mix, lanolin, cocamidopropylbetaine, formaldehyde, corticosteroids, methylchlorisothiazolinone (MCI)/methylisothiazolinone (MI), propylene glycol, and benzalkonium chloride. Upon review of the included studies it was also estimated that between one quarter and one third of children suffering from ACD could potentially benefit from a “pre-emptive avoidance strategy” (P.E.A.S.) of the stated top 10 allergens! Dermatitis Academy then created the Simple & Free guideline to highlight the products devoid of the top 10 sensitizers. Given that benzalkonium chloride (BAC) is a very rare allergen and well known irritant, the high reporting from one study in the meta-analysis likely represents irritant reactions being read as allergens. For this reason BAC was replaced by para-phenylenediamine, a Consumer Patient Safety Commission (CPSC) designated ‘Strong Sensitizer’, in Dermatitis Academy’s top 10 sensitizers to be pre-emptively avoided.
http://www.ncbi.nlm.nih.gov/pubmed/22828255
http://www.ncbi.nlm.nih.gov/pubmed/18503686
By utilizing resources that identify consumer products for the presence, or lack of, specific contact allergens, consumers can use the pre-emptive avoidance strategy to select Simple & Free formulations and potentially prevent the development of, or remit ACD. Patients most likely to benefit from these efforts include those with eczema, sensitive skin, known allergy, or family history of inflammatory skin diseases. This article briefly shows examples of products devoid of the top allergens, but consumers are encouraged to utilize Dermatitis Academy’s Simple & Free guideline, which utilizes the pre-emptive avoidance strategy P.E.A.S. to highlight products that are both Simple in their formulation and Free of the top 10 P.E.A.S. identified sensitizing allergens.
Article:Hill H, Goldenberg A, Golkar L, Beck K, Williams J, and Jacob SE. Pre-Emptive Avoidance Strategy (P.E.A.S.) – addressing allergic contact dermatitis in pediatric populations. Expert Review of Clinical Immunology. 2016 Jan http://www.ncbi.nlm.nih.gov/pubmed/?term=P.E.A.S.
Aerosolized MI
Methylisothiazolinone (MI) is a preservative causing “an outbreak of allergy … which we have not seen before in terms of scale in our lifetime…I would ask the cosmetic industry not to wait for legislation but to get on and address the problem before the situation gets worse,” Dr. John McFadden, dermatologist at St. John’s Institution of Dermatology in London, 2013. Duffin, C., Warning over ‘epidemic’ of skin allergies from chemical in cosmetics and household products, in The Telegraph. It is not just a preservative in personal hygiene products, it is also in cleaning supplies, air fresheners and household paint. Notably, reactions can occur through airborne exposures through aerosolized MI.
Discussion by Phillip Grigsby, BA. MS3 and Sharon Jacob, MD, Loma Linda University School of Medicine and Department of Dermatology
Aerts et al. describe a case of a 4 year-old girl who was believed to have been sensitized by skin exposure to methylisothiazolinone (MI) that was contained in Scottex Fresh® moist toilet paper (Kimberly Clark).1 The child developed a papular eruption (dermatitis) over an erythematous base at the site of the wipe exposure that eventually subsided after application of topical steroids and cessation of exposure to the wipes. Six months later, she had a similar, papular dermatitis involving her face, including nasolabial folds and eyelids, which was morphologically similar to atopic dermatitis in an airborne (exposed area) distribution. It was resistant to more potent topical corticosteroids, and continued to wax and wane for another 4 weeks. The child was epicutaneously patch tested and found to be contact sensitized (immune system recognized) to 25 parts per million (ppm) of MI (well below the levels in both the wipes and paint). In review of exposures, it was noted that her parents painted her room with water-based paint. Analysis showed that the paint contained MI at 53 ppm. Aerosolized MI in the paint was determined to be contributory to the development of the new dermatitis in this MI sensitized child.
http://www.ncbi.nlm.nih.gov/pubmed/23510347
MI was originally formulated as Kathon®, a mixture of methylchloroisothiazolinone (MCI) and MI. It has since been discontinued in the European Union due to high rates of allergic contact dermatitis.2 MI currently is allowed allowed in select products (leave on, rinse off) to 100 ppm. A review of the literature found 21 cases of aerosol-induced (aerosolized MI) dermatitis to MI.3-7 Aerts et al. point out the first child to be confirmed to have this reaction. Of note, a similar case has since been reported where a three year-old girl was sensitized by MI-containing wipes, and later developed an airborne spread allergic contact dermatitis after paint exposure.6 Notably, the mimickry to atopic dermatitis (eczema) increases the risk that this child could have gone mis- or undiagnosed. Patch testing was vital in correctly making her diagnosis of allergic contact dermatitis, with systemic (airborne) activation. It is important to note that MI as a stand alone substrate is not included on the commercially available patch test screening kit. Testing with the MCI-MI combination substrate can miss up to 40% MI reactions, likely because the low concentrations of MI in the tests.8
References
Additional articles that may be of interest (Aerosolized MI):
Airborne exposure to preservative methylisothiazolinone causes severe allergic reactions.
http://www.ncbi.nlm.nih.gov/pubmed/23212711
Generalized allergic contact dermatitis caused by methylisothiazolinone in a spray tan.
http://www.ncbi.nlm.nih.gov/pubmed/26098619
Five cases of severe chronic dermatitis caused by isothiazolinones.
http://www.ncbi.nlm.nih.gov/pubmed/23782361